

A Trauma-Conscious School
At Wildwood Nature School, we’ve come to the understanding that most adults and children in our society have experienced trauma at some point in their lives and haven’t had the experience of releasing this trauma from their bodies. This results in trauma energy becoming ‘stuck’ in the body and being expressed in the form of physical and mental illness, pain in the body and non-social behaviours. This understanding underpins much of how we operate in terms of our relationships with the children, families and colleagues at Wildwood Nature School. Read on to find out a bit more about trauma and what being a trauma-conscious school means.

What is trauma?
One of the world’s leading trauma experts, Gabor Maté, describes trauma in his latest book The Myth of Normal, as follows:
“The meaning of the word ‘trauma,’ in its Greek origin, is ‘wound.’... ‘trauma’ is an inner injury, a lasting rupture or split within the self due to difficult or hurtful events. By this definition, trauma is primarily what happens within someone as a result of the difficult or hurtful events that befall them; it is not the events themselves…trauma is a psychic injury, lodged in our nervous system, mind, and body, lasting long past the originating incident(s), triggerable at any moment….Whether we realise it or not, it is our woundedness, or how we cope with it, that dictates much of our behaviour, shapes our social habits, and informs our way of thinking about the world.”
It can be helpful to remember that, “trauma is not what happens to you but what happens inside you.” The actual facts of an incident are not what causes trauma; instead, trauma occurs when the body’s nervous system is overwhelmed by a specific incident or ongoing experiences.
Another of the world’s most prominent experts on trauma, Peter Levine, the creator of Somatic Experiencing, explains this further by saying, “Trauma is not just what happens to us, but what we hold inside in the absence of an empathetic witness.” Especially for young children, the presence of a caring witness - normally a parent - can mean that even very challenging incidents do not cause lasting wounding. It is the lack of this ‘empathetic witness’ that is so often the cause of nervous system overwhelm and lasting inner injury.
Why is trauma so prevalent?
Apart from more obvious causes of trauma such as abuse and neglect, Peter Levine & Maggie Kline list the many common and everyday experiences that have been proven to traumatise young children. These include:
hospital births and birth complications;
sleep training - leaving babies to cry alone for long periods of time;
extremes of temperature (for small babies);
any medical procedure when the child is too young to understand what’s happening;
falls and injuries;
car, bike and other accidents;
experiencing or witnessing violence, including in the media;
loss – death, separation, divorce, loss of possessions;
witnessing arguing or outbursts of anger;
being bullied by peers.
While this list is not extensive, and there are many other things that can cause trauma, it’s clear that most young children may have experienced one or more events that could have traumatised them, which is why being conscious of the effects of trauma is vital when working with children.
However, as Maté explains, it’s not just specific incidents that cause trauma. “Children, especially highly sensitive children, can be wounded in multiple ways: by bad things happening, yes, but also by good things not happening, such as their emotional needs for attunement not being met, or the experience of not being seen and accepted, even by loving parents.”
What Gabor Maté lays out so beautifully in The Myth of Normal, is that we’re living in a toxic society and culture, one in which nearly everyone is blindly suffering from trauma and where the pressures of everyday life do not in any way support parenting that doesn’t traumatise:
“Our cultural ecology does not support attuned, present, responsive, connected parenting…[T]he destabilisation begins with stress transmitted to infants still in the womb, with the mechanisation of birth, the attenuation of the parenting instinct, and the denial of the child’s developmental needs. It continues with the increasingly intolerable economic and social pressures on parents these days and the erosion of community ties, and magnifies with the disinformation parents receive on how to rear their young. Reinforced by educational systems that too often stress students with pressure to compete, the process culminates in the exploitation of children and youth for the glory of the consumer market.”
The effects of our toxic culture begin in utero - every element of the development of a foetus, including the architecture of its brain, is directly impacted by the mother’s emotional state, nervous system and stress levels. In fact, many would argue that the effects of trauma begin even before an infant is conceived. Each of us has our own legacy of intergenerational trauma that gets handed down to us at the point of conception. Tori DeAngelis describes in an American Psychological Association article the research that has been carried out on descendants of Holocaust survivors and those who survived the starvation of Soviet Ukrainians in the 1930s under Stalin. The intergenerational impacts on those descendants included risky health behaviours, anxiety and shame, food hoarding, overeating and authoritarian parenting styles. Generational trauma can be passed down when an ancestor hasn’t healed their own trauma. But trauma doesn’t need to be the result of genocide to be passed down; the more common causes of trauma (violence, abuse, neglect), if unresolved, will be passed down to our children.
Furthermore, modern day parenting practices such as putting babies to sleep in cots, using buggies, and parents spending most of their day away from their children, are completely in contrast with what babies expect, in evolutionary terms, when they are born. In the 1970s, Jean Liedloff spent years living with the indigenous Yequana tribe in the jungles of Venezuela and studied their child-rearing practices; practices which had been uninterrupted by modern ideas. She was surprised at how peaceful the babies were and how independent the older children were. She developed The Continuum Concept to describe how, evolutionarily speaking, the human brain and nervous system are not much different from our hunter-gatherer ancestors, who lived in tribes until around 10,000 years ago. Babies come into the world with certain evolutionary expectations: to sleep with their parents, as all mammals do, to be breastfed, and to spend at least the first year of their lives in arms (i.e. against their caregivers' bodies in a baby carrier). When infants do not receive the kind of parenting they expect, this evolutionary continuum is broken, which can result in them being traumatised. Given that parenting has moved away from more instinctive styles for at least the past 100 years, it’s fair to say that most of us will not have been raised in a way that honours our evolutionary expectations.
One of a child’s primary and irreducible needs is for attachment to their caregivers. For an infant, this is a matter of survival. However, so often in present day parenting, another of the child’s irreducible needs - for authenticity - is so often subsumed in the name of maintaining the attachment relationship. When babies and young children authentically express their big, loud and messy emotions, parents often don’t have the time or tolerance to allow them. Telling children to be quiet, or to stop crying, or distracting them from difficult emotions, denies them their authentic expression. But because the need for attachment is so strong, children will suppress their emotions, needs and eventually even their own thoughts, in order to stay in attachment with their caregiver. As Maté explains:
“Although both needs [for attachment and authenticity] are essential, there is a pecking order: in the first phase of life, attachment unfailingly tops the bill. So when the two come into conflict in a child’s life, the outcome is well-nigh predetermined. If the choice is between “hiding my feelings, even from myself, and getting the basic care I need” and “being myself and going without,” I’m going to pick that first option every single time. Thus our real selves are leveraged bit by bit in a tragic transaction where we secure our physical or emotional survival by relinquishing who we are and how we feel….
“[A child] can conclude either that the people she relies on for love are incompetent, malicious, or otherwise ill-suited to the task, and she is all alone in this scary world; or that she herself is to blame for, well, everything. As painful as the latter explanation is, it is far preferable to the other one, which paints a life-threatening picture for a young being with zero power or recourse. The first option is not an option at all. Better to believe “It’s my fault; I’m bad,” which lets you believe there’s the chance that “if I work hard and be good, I will be lovable.” Thus, even the debilitating belief in one’s unworthiness, nearly universal among people with mental health diagnoses and addictions, begins as a coping mechanism.”
We can all probably remember times when our parents were too busy or distracted to fully accept and allow our authentic expression, and as parents ourselves, many of us will probably have been in the same position. But this is one cause of early trauma; when our caregivers don’t see us and accept us just as we are, it creates a rupture, and disconnects us from our authentic selves.
It’s hard to imagine that anyone in our society could be totally free of the generational, collective and individual trauma that is so prevalent. Many of us as parents are carrying trauma from our own childhoods and beyond, and our children have probably already experienced trauma, even in their short lives. But what does trauma look like? How can we recognise the symptoms?
What are the symptoms of trauma?
In Trauma Through a Child's Eyes, Peter Levine and Maggie Kline describe 4 categories of symptoms that are identifiable in infants and young children following trauma. These categories are: hyperarousal, constriction, dissociation, and shutdown (freeze). When anyone experiences a threat, the body’s nervous system response is fight or flight. This releases a huge amount of adrenaline into the bloodstream to prepare the larger muscles for either fight or flight. What happens with trauma, is that the individual doesn’t get to complete the cycle of fight or flight. One of the key elements of trauma is a feeling of helplessness, especially for infants and young children who often don’t have the ability to flee or fight. So all of this energy has nowhere to go. And depending on the nature of the trauma, this arousal energy either remains in the body as hyperarousal and constriction, or gets compartmentalised leading to dissociation or shutdown.
Some of the symptoms of hyperarousal include:
rapid breathing
fearful darting eyes
fidgeting and restlessness
easily wound up
night terrors
difficulty falling and staying asleep
hypervigilance
an exaggerated startle response
symptoms normally attributed to Attention Deficit Disorder with Hyperactivity (ADHD)
Some of the symptoms of constriction include:
stiff or awkward appearance
rigid gait
poor coordination
tense neck and shoulder muscles
complaints of tight insides
lack of interest in food and issues with eating
diarrhoea and/or constipation
frequent tummy aches and headaches
shallow breathing or hyperventilation - both can limit oxygen flow to brain causing fatigue and lethargy
Some of the symptoms of dissociation include:
inattentiveness
fatigue
daydreaming
extreme shyness
withdrawal
isolation from peers
Some of the symptoms of shutdown (freeze) include:
numbness
zoning out
vacant look
lack of facial expression
Sometimes, the symptoms of trauma don’t fall easily into one of these categories, and there are more generalised symptoms of the stress caused by the trauma. As Levine and Kline explain, “when a child is suffering from trauma, the brain behaves differently. It may register any novelty or excitement as potentially harmful. This sends a cascade of unneeded chemicals, marching like soldiers to the battleground (to the most primitive parts of the brain), to fight a war that doesn’t exist. It is this continuing pattern of excess energy that creates trauma’s symptoms.”
General symptoms of traumatic stress in young children include:
emotional outbursts and tantrums
separation anxiety and excessive clinginess
anger
throwing toys
aggression - hitting or bullying others, biting, grabbing and kicking
intense anxiety and worry
regressive behaviours returning to an earlier stage of development e.g. bed-wetting, baby-talk
lack of ability to concentrate, finish tasks or process new information
Levine and Kline explain that all of these bodily responses to trauma are survival and defence mechanisms that in some way protect the individual. The residual, often negative, symptoms are because this powerful survival energy hasn’t been released; it’s only meant to be a short-lived, temporary measure since fight or flight is metabolically costly. For example, the constriction and tensing of muscles as part of the preparation for fight or flight are essential. But when the individual doesn’t get to use this fight/flight energy, it remains not only in the muscles, but also the joints, internal organs, sensory and respiratory systems, hence many of the digestive symptoms associated with constriction.
Another example of the immediate short-term benefits of these bodily responses, is with injuries and falls: the freeze response actually spares the child from the initial impact through physiological shock and dissociation and the temporary numbing from the release of opiates such as endorphins and epinephrine. But as Levine and Kline explain, “Immobility, freeze, helplessness, and dissociation are involuntary psycho-physiological reactions to overwhelm. They are meant to be time-limited.”
Levine and Kline give 2 examples below of how trauma can have such an impact on children and how this often translates to issues with learning:
“Disruptions in visual processing are characteristic of students who have been traumatised. For many who have witnessed or been involved in the horror of a violent attack or an accident, the wide-eyed look of terror remains as if frozen in time. Sometimes it is simply a blank expression. When the chaos is random and chronic, eyes will tend to wander to the sides to broaden the peripheral field of vision as a function of hypervigilance, or standing guard. Children who saw the danger coming directly at them may experience a momentary visual ‘freeze’ at certain triggering angles as their eyes glide across a page of print. For some students, the left-to-right movement across the page becomes stressful, leading to fatigue after reading…Often traumatised students are labelled as learning disabled or dyslexic because of lack of ability to track smoothly with both eyes.”
“When students have experienced trauma that involves encounters with gravitational forces and velocity, such as falls, vehicular accidents, and sporting injuries, they may have impaired access to their natural protective reflexes and balances. They are then more likely to sustain repeated injuries or be ‘accident-prone’…Students with undeveloped or ‘frozen’ reflexes are more susceptible to learning problems, especially with reading and writing. Activities that improve balance and motion have significant effects on visual processing and academics.”
What are the long-term effects of trauma?
Trauma causes long-lasting physiological changes in the brain which can lead to a whole host of problems. As Gabor Maté argues, the rapid rise in mental health and autoimmune illness in society that we’ve seen over the past 50 years is caused by unresolved trauma. The main cause of this is the inflammatory response of the immune system during and after traumatic experiences. Sadly, most trauma is experienced during infancy, when the effects are most pronounced and long-lasting. Peter Levine and Maggie Kline describe just how wide-reaching the effects can be:
“What happens from the foetal period until two years of age creates the blueprint that influences every system in the body from immunity to the expression and regulation of emotion, to nervous system resilience, communication, intelligence, and self-regulatory mechanisms for such basics as body temperature and hormone production…[When an infant suffers trauma] the growing brain organises itself to be more reactive to survival functioning at the expense of development in the limbic and cortical areas responsible for the modulation of impulse and emotion.”
Gabor Maté describes how trauma limits our response flexibility - “the ability to choose how we address life’s inevitable ups and downs, its disappointments, triumphs and challenges.” Response flexibility is a function of the midfrontal portion of our cerebral cortex; we’re not born with this skill, it develops over time. Early trauma can seriously impact upon the brain circuits that govern response flexibility causing an individual to become “stuck in predictable, automatic defensive reactions, especially to stressful stimuli…The past hijacks and co-opts the present, again and again.” Dan Siegel and Tina Bryson use a wonderful visual of the “upstairs” and “downstairs” brains (explained in more detail here) to describe how the evolutionarily older downstairs brain can hijack the more evolved upstairs brain as a result of trauma. They call this “flipping your lid” and use the below image of the hand model of the brain to help teach children about their brains.

Taken from The Whole-Brain Child by Dan Siegel and Tina Payne Bryson
Physical illness, mental illness, learning difficulties, issues with self-regulation… the list of long-term effects of trauma is long and this is why it’s so important to resolve trauma, especially in children. One of the saddest effects of trauma is the power it has to constrict our physical and psychological selves. Gabor Maté says that unresolved trauma “constrains our inborn capacities…keeps us stuck in the past, robbing us of the present moment’s riches, limiting who we can be.” Furthermore, trauma can keep us isolated. Prentis Hemphill, founder of The Embodiment Institute, said at the 2022 Collective Trauma Summit, “Trauma interrupts relationship; in our own body and also with other beings, with human beings and beings in our ecosystem.” Maybe the more recent epidemic of loneliness that we hear about has also been created, in part, by the unresolved trauma that exists in our society.
Trauma can seriously impact upon our ability to feel and express the full range of our emotions; one of our irreducible needs in childhood as defined by Gabor Maté. And again, this may be one of the ways in which trauma leads to isolation and loneliness. As described above, parents often shut down a child’s natural emotional response, one that might seem overblown to the triggering event. But what that experience does is crystallise in your heart as an emotion that’s not safe to feel, one that could jeopardise your relationship with others. This isn’t a conscious choice, but an involuntary survival mechanism. However, repeated experiences like this can lead to a total inability to feel emotions and to become hardened. As Gabor Maté and Gordon Neufeld so beautifully express:
“Our emotions are not a luxury but an essential aspect of our makeup. We have them not just for the pleasure of feeling but because they have crucial survival value. They orient us, interpret the world for us, give us vital information without which we cannot thrive. They tell us what is dangerous and what is benign, what threatens our existence and what will nurture our growth. Imagine how disabled we would be if we could not see or hear or taste or sense heat or cold or physical pain. To shut down emotions is to lose an indispensable part of our sensory apparatus and, beyond that, an indispensable part of who we are. Emotions are what make life worthwhile, exciting, challenging, and meaningful. They drive our explorations of the world, motivate our discoveries, and fuel our growth. Down to the very cellular level, human beings are either in defensive mode or in growth mode, but they cannot be in both at the same time. When children become invulnerable, they cease to relate to life as infinite possibility, to themselves as boundless potential, and to the world as a welcoming and nurturing arena for their self-expression.”
Polyvagal theory
Stephen Porges, a psychologist and neuroscientist, developed the Polyvagal Theory, a “science of safety”, to describe how trauma affects the body and various corresponding approaches to healing. His focus is on the vagus nerve, or wandering nerve, a part of the autonomic nervous system. The vagus nerve originates in the brain stem and has 2 parts: the ventral (front) and dorsal (back). The ventral vagus travels through the vocal cords, heart and lung, while the dorsal vagus travels below the diaphragm to the viscera. While the vagus nerve has traditionally been associated with the parasympathetic branch of the autonomic nervous system and its positive attributes of “rest and digest”, Porges highlights that not all parasympathetic responses are restorative. When the dorsal ventral vagus takes over, it can lead to dangerous slowing of the heart rate and shutdown of key organs.
In evolutionary terms, and in foetal development, the dorsal vagus is older and the ventral vagus more recently developed. All vertebrates have a dorsal vagal nerve and it corresponds to the more primal survival strategies seen in reptiles and amphibians of freeze and immobilisation. The ventral vagal nerve developed around 220 million years ago, when mammals evolved. It’s closely linked with breastfeeding and more complex and sophisticated responses. In utero, the ventral vagus system develops at around 32 weeks, so babies born very prematurely will only have access to a defensive state and might struggle with breastfeeding.
The key tenet of Porges’ theory is that it is our social engagement system, enabled by the ventral vagus, that allows us to feel safe. Social engagement includes voice tone, prosody, facial expression and head gestures because it developed out of the same structures used for sucking, swallowing and breathing that babies use in breastfeeding. At the Biology of Trauma Conference in 2022 he said, “We must reclaim our evolutionary heritage of feeling safe with others.” The ventral vagal nerve is myelinated (insulated) so is more efficient and can lead to rapid firing, whereas the dorsal vagal nerve is unmyelinated. So the ventral vagal system should be the faster one to turn on, but traumatic experiences can cause a dissolution of the evolutionary/developmental structures, causing the dorsal vagus to take over.
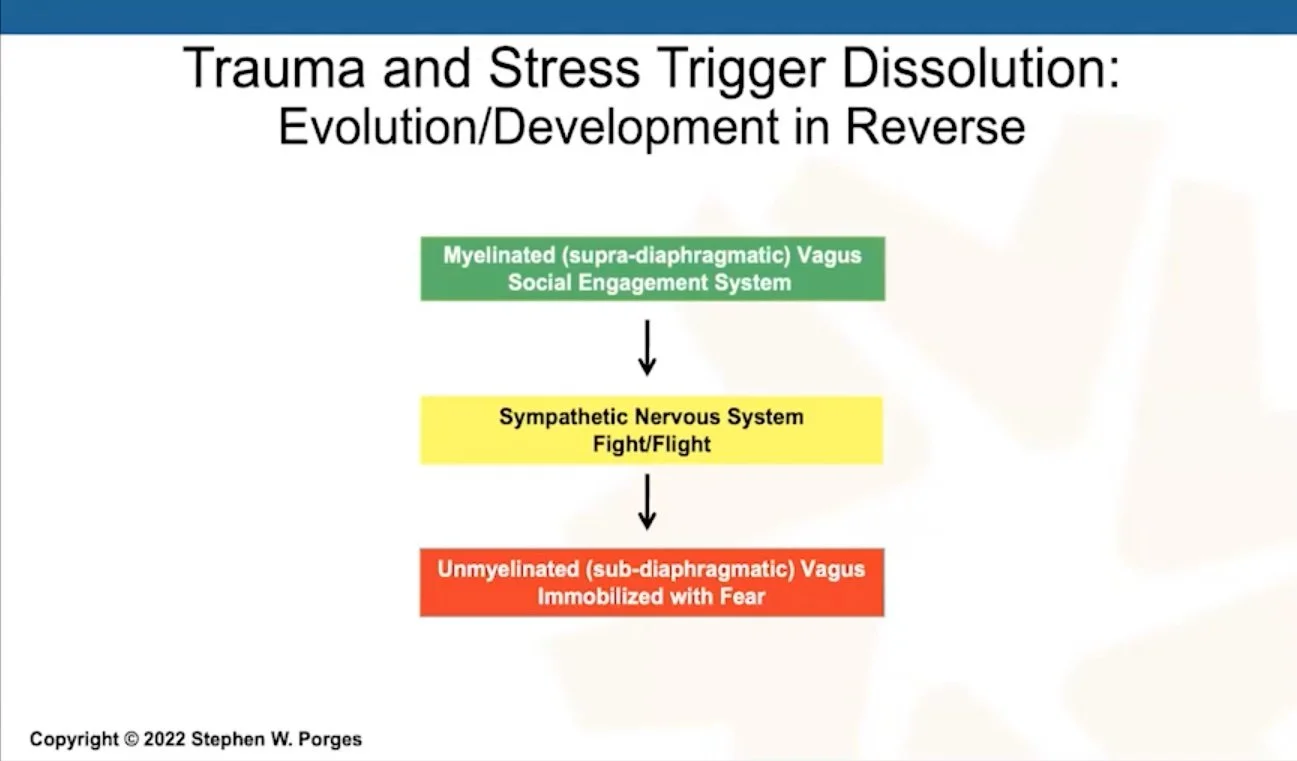
Taken from Stephen Porges’ presentation at the NRBS Conference 2022
Traumatic experiences and chronic stress retune the autonomic nervous system into a defensive state that:
Disrupts homeostasis functions leading to illnesses such as irritable bowel syndrome and fibromyalgia;
Biases experiences towards detecting stress - our physiological state is the intervening variable between stimuli and response i.e. it’s not just the stimulus but how our nervous system makes us perceive stimuli;
Limits opportunities to establish safe, trusting relationships.
The ventral vagal system leads to social engagement, turns off threat reactions, fosters calmness, sociality, connectedness, health, optimises oxygen diffusion into the blood, and supports homeostasis. Whereas the dorsal vagal system leads to immobilisation, poor eye contact, difficulties in social communication, blunted facial expressions, difficulties in behavioural state regulation (hypervigilant, anxious, distractible, impulsive, tantrums, hypoarousal), difficulties in listening and following verbal commands, speech-language delays, sound sensitivities and illnesses related to the internal organs, particularly the digestive system.
Porges argues that we need to honour what the body does to protect us rather than judge it, as this just creates shame and makes the freeze / dissociation / constriction response worse. But we must do activities that support our healing; primarily ones that engage the ventral vagus system. One such activity is singing. Singing uses vocalisation and facial muscles thereby stimulating the ventral vagus. If singing is done with others, then this leads to social engagement. Porges is a huge proponent of co-regulation - when a caring other helps an individual to regulate. Activities such as singing, or any other social activity, even just a kind face and soothing tone of voice, can dramatically support an individual to come back into a feeling of safety. At the Collective Trauma Summit in 2022 he said, “We need to feel safe enough to enable our innate problem-solving capabilities, creativity and benevolence.”
What can we do to heal trauma?
Bessel van der Kolk states that “all trauma is preverbal.” By this, he means that trauma either impacts the brain in utero or during infancy before language has developed; or that traumatic events often bypass the parts of our brain that control language. This is why traumatic memories are normally fragmented images, sounds and sensations rather than coherent narratives. It can be hard for even highly verbal adults to be able to describe trauma until they’ve processed and released it.
Furthermore, Peter Levine and Maggie Kline argue that “trauma resides in our biology, not primarily in our psychology…[therefore the core symptoms of trauma] must be released through the body.” In order to regain our “instinctual wisdom”, we must heal through our bodies and learn from our animal friends. “[A]nimals have a built-in ability to rebound from a steady diet of danger. They literally ‘shake off’ the residual energy through trembling, rapid eye movements, shaking, panting, and completing motor movements…taking deep spontaneous breaths” once the body has returned to equilibrium. Human beings naturally do this too; however, this ability to ‘shake off’ trauma has somehow been lost.
Based on years of study, of both the animal and human word, Peter Levine developed his therapeutic modality, Somatic Experiencing (SE). It’s a bottom-up approach because it works with bodily sensations first. SE therapists carefully work with individuals to support their body to complete bodily movements that were interrupted by trauma, to identify parts of their body that contain stuck energy, and to create a sense of safety for individuals that allows the natural shaking that heals the body from trauma. He advises though that the key in working with trauma and sensation is to titrate gently and slowly to release energy one small bit at a time. Otherwise, the quick release of all that stuck trauma energy can be scary and lead to contraction again. There are elements of SE that can be used to work with children to help them to release this stuck energy.
In a recent conference, Peter Levine explained the importance of movement throughout the day to regulate the nervous system. When this is done with the teacher, it’s co-regulation. Why co-regulation is so powerful, as alluded to by Stephen Porges, is that, especially for babies and young children who can’t self-regulate, co-regulation eventually leads to the ability to self-regulate. It supports connection to oneself in the present moment in an embodied way.
Another vital healing modality is play. Gabor Maté says, “All young mammals play, and for critical reasons. As the neuroscientist Jaak Panksepp identified, we have a designated “PLAY” system in our brains in common with other mammals. Play is a primary engine of brain development and is also essential to the emotional maturation process.” The benefits of play are enormous (read more about play here), but in terms of healing from trauma in particular, play allows for social engagement, touch, bonding, physical release, processing emotions through re-enactment of traumatic events, and practise establishing boundaries. Levine and Kline explain:
“As children ‘chase’, ‘flee’, ‘escape’, ‘make boundaries’, ‘run to a safe place’, and ‘feel strength and power in their limbs and belly,’ they are forming new neural pathways that support resiliency and self-regulatory capacities. Sensory experiences through play are what build neural networks to repair trauma most efficiently…Sensory-motor input has a direct effect on the reptilian survival brain…What children need in order to feel whole rather than frightened is a sense of safety, connection, grounding, and the actual experience of defending their boundaries or fleeing from danger.”
Levine and Kline also examine how play provides children an opportunity to regain their balance and resilience, to discharge intense mobilisation energy and to express their thoughts and emotions freely. It’s very common for children to repeatedly re-enact a traumatic experience in their play, and with guidance, this can be incredibly healing. They explain that children often engage in compulsive, repetitious, re-enactment of trauma through play but most children will attempt to avoid the traumatic feelings that their play evokes. Re-working or renegotiation of a traumatic experience through play, allows for resolution, and with guidance, the child can gradually and sequentially master their fear and other feelings.
As all of this research suggests, being a trauma-conscious school in this day and age is essential. We’ve utilised all of the deep learning from these great psychologists, neuroscientists, doctors and researchers to develop our own methodology to support children to understand and release trauma. Below are some of the ways that we do this at Wildwood Nature School:
We respond to each child with the understanding that their behaviours are a nervous system response and are often beyond their conscious control;
We take a proactive approach by facilitating particular activities and games that help the nervous system to release stuck trauma from the body;
We teach children how to feel sensations in their body and techniques to be able to ground themselves and allow sensations and natural releases to occur when they experience heightened emotions or an event that could cause trauma;
We give them the language to be able to express the wide range of their sensations, feelings and emotions;
We sing and dance together;
Our adults are always aware of their tone of voice and facial expressions so that they constantly convey safety to the children and encourage the social engagement system to turn on;
Our adults are always available to co-regulate alongside the children;
We dedicate a large portion of the day to uninterrupted free play;
We explicitly teach children about trauma and what it means;
We teach children, through games and other activities, how to determine their own boundaries, how to securely express their boundaries and say “no”, so that they are less vulnerable to abuse.
References
DeAngelis (2019) The legacy of trauma: An emerging line of research is exploring how historical and cultural traumas affect survivors’ children for generations to come. American Psychological Association https://www.apa.org/monitor/2019/02/legacy-trauma [accessed 7/03/23].
Hemphill, P. (2022, 8-14 August) The Story Being Told Through Our Collective Body [Conference presentation]. The Biology of Trauma 2.0 Conference (online).
Levine, P. A. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness. North Atlantic Books.
Levine, P. A. & Kline, M. (2019) Trauma Through a Child’s Eyes: Awakening the ordinary miracles of healing - Infancy through adolescence. (2nd ed.) Berkeley: North Atlantic Books.
Levine, P. A. (2022, 8-14 August) Authenticity [Conference presentation]. The Biology of Trauma 2.0 Conference (online).
Levine, P. A. (2022, 28 September - 6 October) Regulating the nervous system with Somatic Experiencing [Conference presentation]. 47th Annual NRBS Conference, Coping with Stress in Today’s World: Solutions for Anxiety, Burnout, and Depression (online).
Liedloff, J. (1986) The continuum concept: In search of happiness lost. (Revised ed.) London: Penguin Books.
Maté, G. with Maté, D. (2022) The Myth of Normal: Trauma, illness and healing in a toxic culture. London: Vermilion.
Maté, G. & Neufeld, G. (2019) Hold on to your kids: Why parents need to matter more than peers. London: Vermilion.
Neufeld, G. (2021) Child-rearing that does not traumatise [Conference presentation]. https://wisdomoftrauma.com/hub/ [accessed 12/10/21]
Porges, S. (2022, 8-14 August) Polyvagal Theory [Conference presentation]. The Biology of Trauma 2.0 Conference (online).
Porges, S. (2022, 28 September - 6 October) Creating Environments of Safety and Trust Through Polyvagal Theory [Conference presentation]. Collective Trauma Summit 2022 (online).
Porges, S. (2022, 21 October) Applications of the polyvagal theory [Conference presentation]. 47th Annual NRBS Conference, Coping with Stress in Today’s World: Solutions for Anxiety, Burnout, and Depression (online).
Siegel, D. J. & Bryson, T. P. (2012) The Whole-Brain Child: 12 proven strategies to nurture your child’s developing mind. London: Robinson.
Van Der Kolk, B., MD. (2015). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Penguin Books.
